Introduction and objectives
To describe our off-clamp robot-assisted partial nephrectomy (RAPN) and to evaluate perioperative and functional outcomes stratified by tumor size and PADUA classification.
Methods
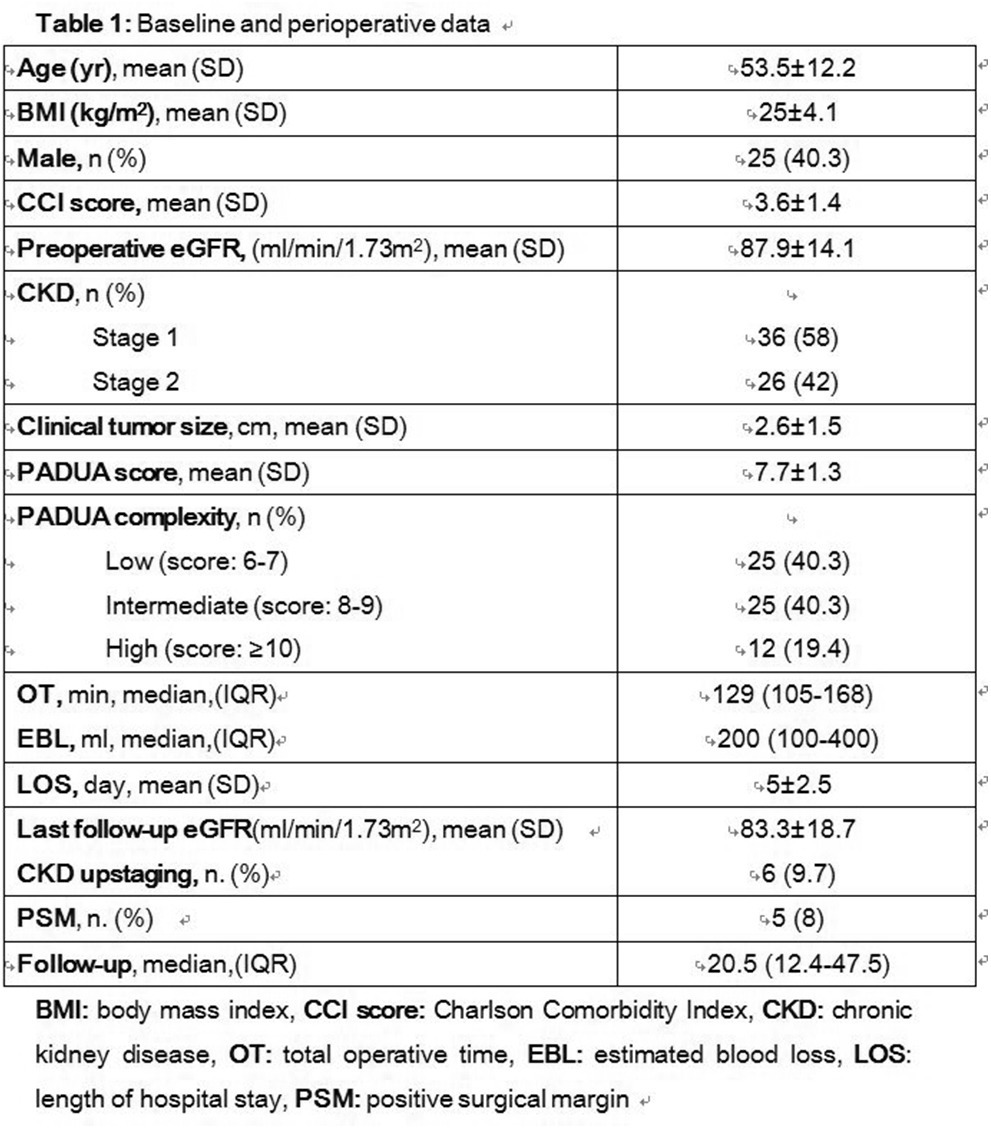
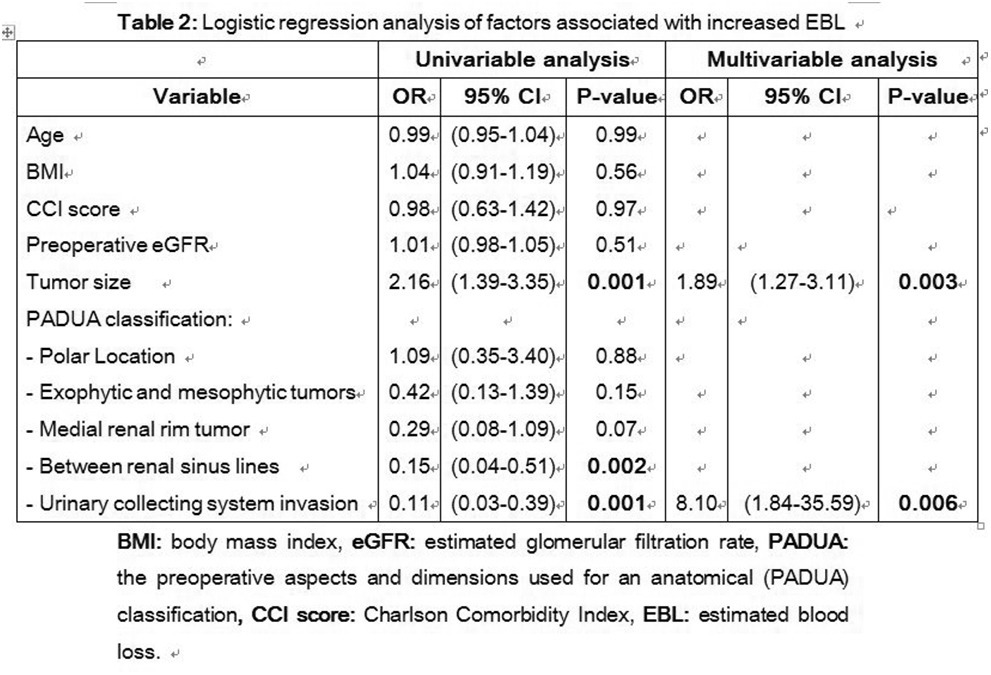
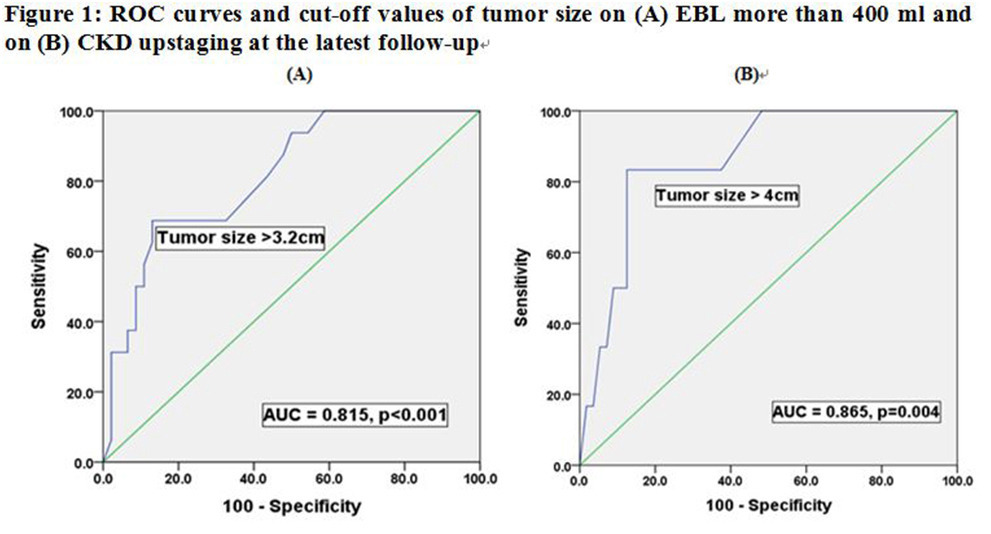
Retrospective analysis of 62 patients who underwent off-clamp RAPN from September 2006 to January 2016 was performed. Increased estimated blood loss (EBL) was defined as intraoperative bleeding more than the 75th percentile. ROC analysis was used to determine the optimal threshold of tumor size for both increased EBL and chronic kidney disease (CKD) upstaging. Multivariable analysis was used to assess risk factors for increased EBL.
Results
Mean patients age was 53.5 years and mean tumor size was 2.6 cm. ROC analysis showed that tumor size of 3.2cm and 4cm were cut-off values for increased EBL (AUC=0.82, p4cm) was (97.1% and 51.4%, retrospectively, p<0.001).
Conclusions
Off-clamp RAPN can be safely performed in the hands of expert robotic surgeons; however, risk of intraoperative bleeding in order to achieve good functional outcomes must be adequately balanced before surgery for maximal patient’s safety. Our findings showed that tumors >3.2cm and those involving the urinary collecting system are associated with risk of increased intraoperative bleeding, while tumors >4cm have increased risk of CKD upstaging despite zero ischemia.