Introduction and objective
American Urologic Association guidelines prioritize nephron-sparing in patients with pre-existing chronic kidney disease (CKD). However, there have been few studies directly comparing long-term renal function in patients with pre-operative severe CKD who undergo partial nephrectomy (PN) versus radical nephrectomy (RN). Herein, we compare the risk of progression to end-stage kidney disease (ESKD) following PN and RN among patients with pre-operative stage 4 CKD.
Methods
Patients with stage 4 CKD who underwent PN or RN from 1970-2018 were identified in our institutional registry. Stage 4 CKD was defined as pre-operative eGFR 15 to 29 ml/min/1.73m2. ESKD was defined as initiation of long-term dialysis, kidney transplantation, or sustained post-operative eGFR <15. Patients were followed annually to assess for ESKD. Cox proportional hazards regression analyses accounting for the competing risk of death were used to evaluate associations with progression to ESKD. Surgical complications were categorized according to the Clavien-Dindo classification.
Results
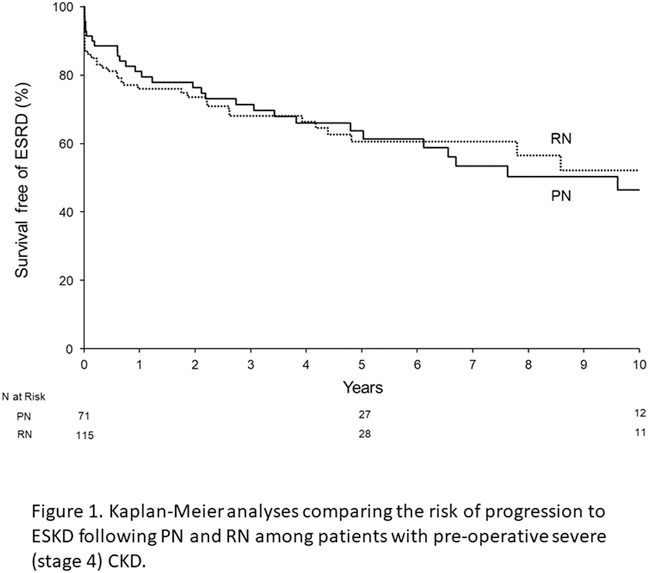
A total of 187 patients with pre-operative stage 4 CKD underwent PN (n=71; 38%) or RN (n=116; 62%) for renal neoplasms with median follow-up 7.2 years (interquartile range 3.8-14.1). Seventy patients progressed to ESKD, including 30 after PN and 40 after RN (Figure 1). In a multivariable setting, older age at surgery (hazard ratio [HR] for 5-year increase 0.81, 95% confidence interval [CI] 0.73-0.91, p <0.001) and higher preoperative eGFR (HR for 5-unit increase 0.68, 95% CI 0.49-0.93, p=0.02) were both associated with lower risk of progression to ESKD. There was no statistically significant difference in the risk of progression to ESRD between PN and RN on adjusted analyses (HR 0.71, 95% CI 0.43-1.18, p=0.18), nor were there significant differences in rates of positive surgical margins, any complication, or Clavien grade 3 or higher complications (21% vs 18%, p=0.6) between PN and RN.
Conclusions
Among patients with pre-operative severe (stage 4) CKD, older age and higher preoperative eGFR were both associated with lower risk of progression to ESKD. We did not observe a significant difference in ESKD progression between PN and RN. These findings should be considered during shared decision-making for renal neoplasms in patients with severe CKD.